Holding governments accountable: Canada’s progress on viral hepatitis elimination

In May 2021, Action Hepatitis Canada (AHC) released its Progress Toward Viral Hepatitis Elimination in Canada 2021 Report. Five years earlier, in May 2016, Canada had signed on to the World Health Organization’s (WHO) first-ever Global Viral Hepatitis Strategy with the goal of eliminating viral hepatitis as a public health threat by 2030. With both a cure for hepatitis C (HCV) and a vaccine for hepatitis B (HBV), this seemed to be a very realistic goal within a reasonable timeframe. But five years on, we had important questions about how Canada was really doing as time was ticking on.
Why a progress report?
The Government of Canada has always been clear that, given the jurisdictional responsibility for healthcare in this country, provinces and territories will be accountable to their citizens to meet the WHO target, not the federal government. Since AHC’s mandate is to ensure government accountability to communities regarding the 2030 commitment, this progress report is a tool that our many members and allies can use to hold governments at provincial and federal levels accountable.
The progress report is also an opportunity to provide annual treatment targets to the provinces and territories, along with policy recommendations to reach those annual targets.
Through a health equity lens
As a coalition of community-based organizations, AHC approaches viral hepatitis using a social justice and health-equity lens. Viral hepatitis affects a number of populations that have been historically marginalized by mainstream healthcare, creating additional hurdles to equitable prevention, testing and treatment services. Our progress report references the five priority populations and one age cohort that are disproportionately affected by hepatitis C as identified in the Blueprint to inform hepatitis C elimination efforts in Canada. These populations are:
|
|
|
|
|
|

Without addressing the inequities in healthcare access for remote and rural areas of Canada, for people who use drugs and/or experience incarceration, and without a reconciliatory approach to healthcare for Indigenous people, considerable barriers to achieving hepatitis C elimination will remain. Our recommendations to the federal, provincial, and territorial governments, and all corrections services, reflect this.
Six metrics to measure our progress
In designing the progress report, AHC selected these six metrics based on the availability of data, as well as the centrality of the target to overall elimination goals:
|
|
|
|
|
|
Current status
Using these metrics, we found that seven out of the ten provinces are on track to meet Canada’s viral hepatitis elimination goals. We did not have enough data to determine the status of the three territories.

Further findings of interest
- With the exception of Saskatchewan, provinces that are achieving their annual hepatitis C treatment targets have implemented HCV RNA reflex testing, which is the practice of automatically testing HCV antibody-positive samples for genetic material (RNA) at the lab. This means that chronic hepatitis C infection can be confirmed in one step, rather than requiring patients to come back for multiple appointments before they are diagnosed. We likely would not have understood the significance of RNA reflex testing in elimination goals without being able to do a side-by-side, province-by-province comparison of treatment counts and testing policies.
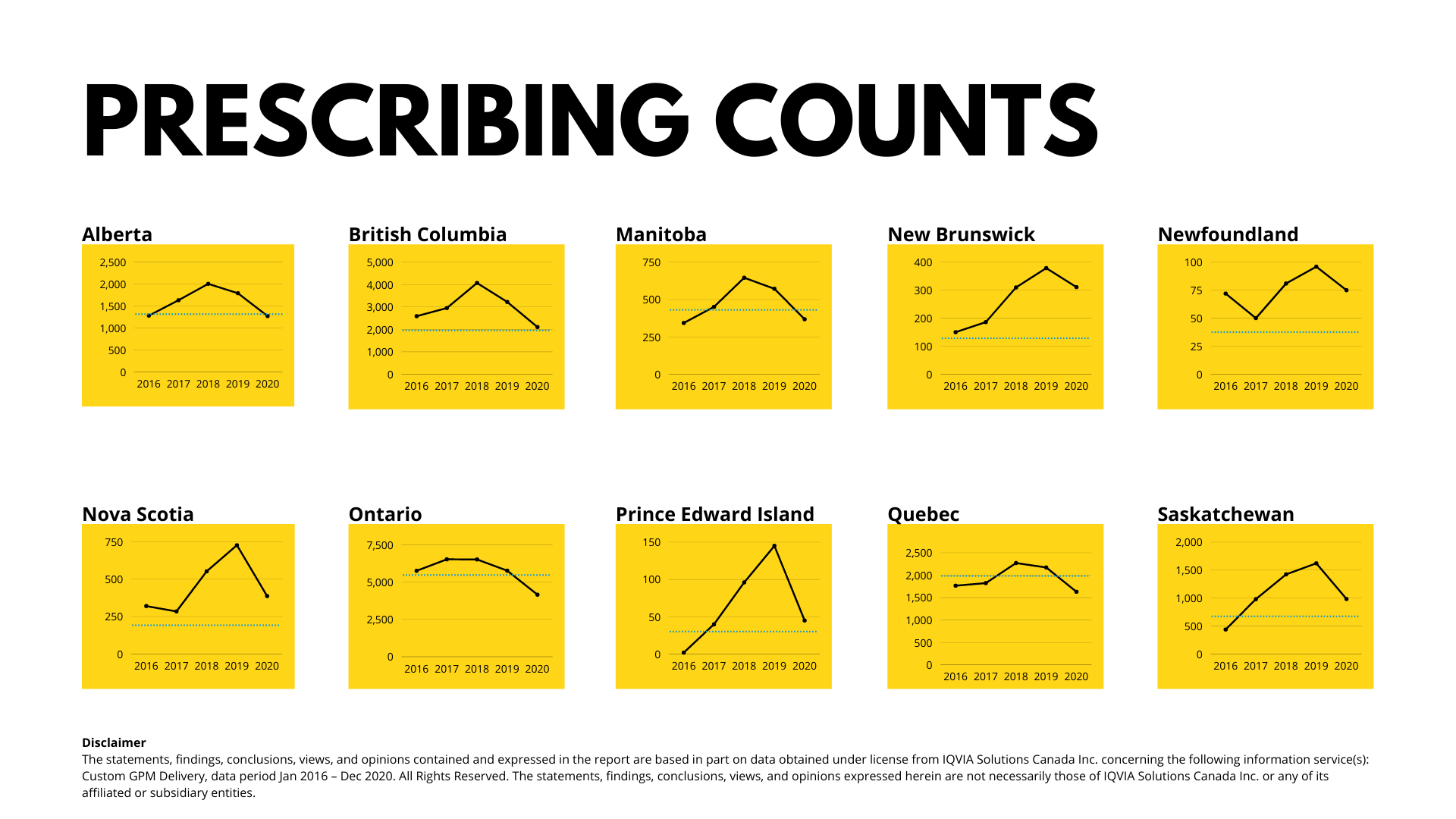
- The rise and fall of annual hepatitis C treatment prescribing counts were not uniform from one jurisdiction to another and seem to correlate with individual governments’ policy changes related to direct-acting antiviral medication reimbursement restrictions. Each province’s prescribing count chart, illustrated in the charts below, is a unique shape, highlighting the impacts of local policy choices. (The black line plots prescribing counts from 2016-2020. The blue line indicates the annual treatment target for each province.)
- Notably, every province saw a drop in hepatitis C prescribing counts in 2020, most likely related to COVID-19 restrictions and shifts in healthcare focus. Many provinces already saw declining numbers of hepatitis C treatment dispensations prior to 2020, so concerted efforts will be needed to get back on track for HCV elimination after COVID-19 pandemic restrictions are lifted.
Data gaps
- While there are internationally recognized hepatitis C research outputs from across Canada, tracking HCV prevalence at the sub-national level across the country is still challenging. As a result, it was difficult to determine what the annual hepatitis C treatment initiation target for each province and territory should be, as there are few recently published sub-national prevalence estimates.
HCV and HBV prevalence estimates should be updated urgently for all provinces and territories. The most recent ones publicly available for most provinces and territories are from 2007.
- The hepatitis C prescribing count data in our report is based on data from select pharmacies which are then modelled to represent dispensations for the entire province. As a result of the limitations of this type of data, they slightly over- and under-estimate the number of patients in different provinces. Also, there were no prescribing count data available for the territories. As the majority of hepatitis C treatments are covered by publicly funded drug plans in Canada, hepatitis C treatment count data should be available from the ministries overseeing these tax-payer-supported drug plans, rather than needing to rely on modelled data that comes with many caveats.
Good data will be key to measuring our progress. How will we know if we have eliminated viral hepatitis in 2030 without accurate data to prove it?
While this report is the first of its kind in Canada, it won’t be the last. We’re already hearing from colleagues who work in this field about the importance of tracking data and holding governments accountable — and how helpful this progress report will be in pursuit of those goals.
Learn more
Download the report to learn more about how your jurisdiction is doing, and what recommendations might be helpful in your own advocacy.
Still have questions or have research that can help inform our next report in two years’ time? Please email us at actionhepatitiscanada@gmail.com.
Jennifer van Gennip is the Coordinator for Action Hepatitis Canada. She lives in Barrie, Ontario, and specializes in advocacy communications for non-profits.