Understanding prescribing trends for hepatitis C treatment in Ontario
The introduction and wide availability of direct-acting antivirals (DAAs) as a treatment for hepatitis C through a phased rollout from 2015 to 2018 held the promise of expanded access to treatment. These simpler treatments carried fewer clinical restrictions and required less specialist support, opening the possibility for primary care providers to treat their patients with hepatitis C. Given barriers to healthcare access for people who use drugs, those of us at the Toronto Community Hep C Program were curious to find out if this had in fact happened.
We collaborated with the Ontario Drug Policy Research Network to investigate this issue, with funding from the Applied Health Research Question program at the Ontario Ministry of Health.
This inter-professional collaboration, involving researchers, people with lived experience and healthcare providers, explored patterns of DAA reimbursement through Ontario’s public drug programs from public records.
Examining these prescriber patterns and this demographic information allowed us to understand who was being prescribed hepatitis C treatment, some of the remaining gaps, and ways that hepatitis C treatment access could be improved for people who use drugs.
What we discovered
Through a cross-sectional study, we looked at prescription DAA claims reimbursed by the public drug program in Ontario (Ontario Drug Benefit) from January 1, 2012 to December 31, 2018. We found that 27,116 people were prescribed treatment from January 2012 until December 2018 (represented in the graph below). Nearly half (n=12,521; 46.2%) of all DAAs were prescribed by gastroenterologists and hepatologists, followed by infectious disease specialists (n=5,292; 19.5%), other specialties (n=4,714; 17.4%) and general practitioners (n=2,481; 9.1%).
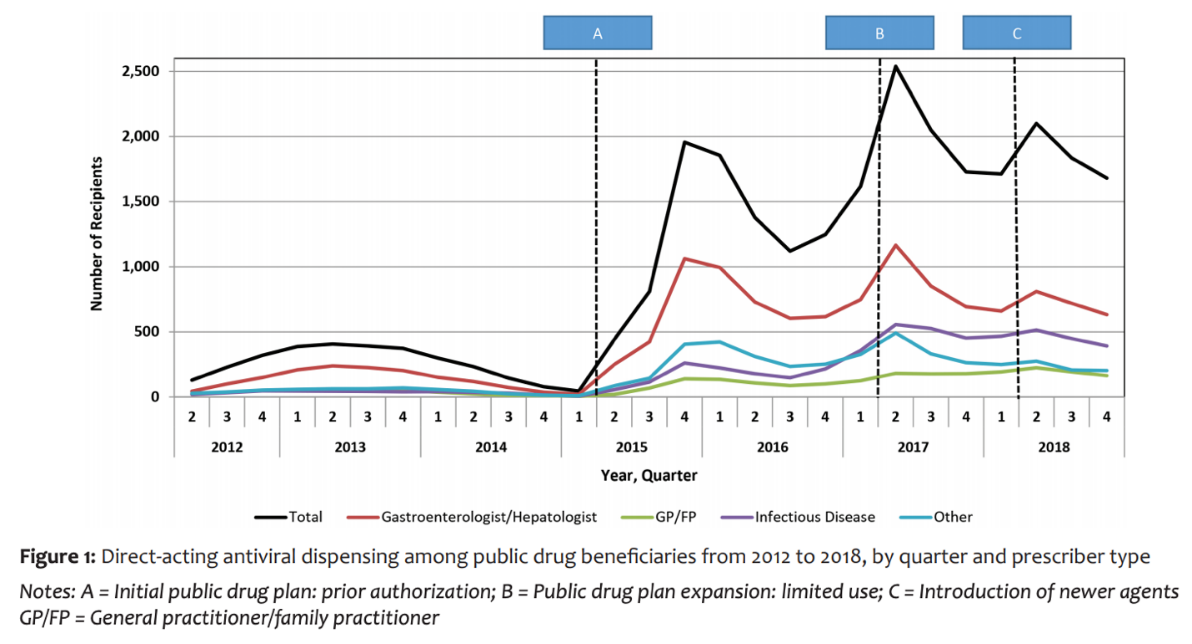{kind=link}
Review of these data also allowed us to understand the demographics of who received these prescriptions. Patients receiving their hepatitis C treatment from gastroenterologists and hepatologists were more likely to be aged older than 65 years or to belong to the top two quintiles of neighbourhood socio-economic status, while patients who received treatment from a general or family practitioner were more likely to have a mental health diagnosis or to be receiving opioid agonist therapy.
Given the challenges that marginalized groups face in attending appointments with specialists, we were concerned to see that most hepatitis C treatment is still being provided in highly specialized medical care settings, which are not as likely to provide care to people who use drugs. These findings are alarming given the fact that most new hepatitis C infections in Canada occur in people who use drugs.
Future research and recommendations for practice
These results are important to consider as we work towards the World Health Organization’s goal of eliminating hepatitis C as a public health threat by 2030, including adopting program recommendations for people who use drugs outlined in the Blueprint to Inform Hepatitis C Elimination Efforts in Canada. New medications have made hepatitis C treatment shorter, easier to administer and more successful, but these benefits have not been fully realized.
While we are happy that prescriptions increased overall, and we applaud the work of specialists prescribing DAAs, we also want to see the expansion and continued support of community-based family doctors and nurse practitioners providing wrap-around treatment and care to people who use drugs and other marginalized populations.
Want to read more?
If you want to know more about our findings, you can read a plain-language summary or the full publication of our research paper.
Mary Guyton is a registered nurse with the hepatitis C team at the Sherbourne Health site of the Toronto Community Hep C Program.
Jennifer Broad works at the Toronto Community Hep C Program.
Kate Mason is a researcher with the Toronto Community Hep C Program.